Meenakshi Radiology
Phone: +91 82485 90535
Address: Near New Bus stand, Tanjore
Specialities
Procedure
Publications
Residents Column
Events
Contact
Liver Interventions
Meenakshi Radiology
Specialities
Liver Interventions
We welcome
Our first batch of DNB Radiology students in Meenakshi hospital, Tanjore
Minimally Invasive Image-Guided Therapies
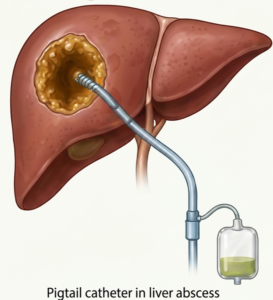
1. Liver Abscess Drainage (Percutaneous)
Technique
Patient in supine position. US/CT guidance.
Local anesthesia.
Needle puncture into abscess under real-time imaging.
Guidewire insertion.
Tract dilatation.
Drainage catheter placement (pigtail or multipurpose).
Aspiration of pus and catheter connected to drainage bag.
Catheter flushed regularly and removed when output minimal and cavity collapsed.
Indications
Pyogenic liver abscess (solitary or multiple)
Amoebic liver abscess (large or non-responding to medical therapy)
Abscess not accessible endoscopically
Sepsis not responding to antibiotics
Contraindications
Uncorrected coagulopathy
Lack of safe percutaneous access
Multiple small abscesses (<3 cm) responding to antibiotics
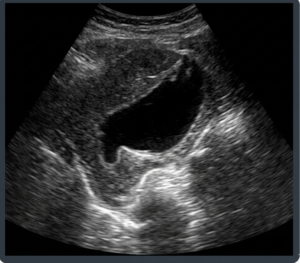
IMAGING
USG: Abscess
CT: Catheter in abscess
Advantages of Liver Abscess Drainage
High success rate (85-95%)
Minimally invasive, safe and effective
Short hospital stay, cost effective
Can be done under local anesthesia
Can be repeated if needed
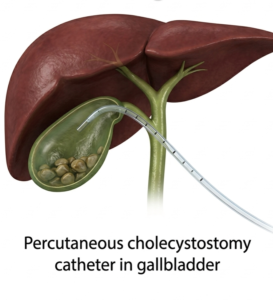
2. Percutaneous Cholecystostomy (Pc)
Technique
Patient supine, right side up.
USG guidance.
Local anesthesia.
Transhepatic or transperitoneal puncture of gallbladder.
Guidewire insertion.
Tract dilatation.
7 Drainage catheter placement (8-12 Fr pigtail).
Bile aspiration and catheter connected to drainage bag.
Catheter removed after clinical improvement (usually 3-6 weeks).
Indications
Acute cholecystitis in high-risk surgical patients
Critically ill/unfit for surgery
Sepsis due to gallbladder infection
Bridge to surgery
Contraindications
Uncorrected coagulopathy
No safe percutaneous window (intervening bowel)
Gallbladder perforation with generalized peritonitis
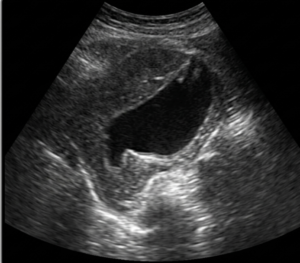
IMAGING
USG: Distended GB
PC catheter in GB
Advantages of PC
Effective decompression and sepsis control
Alternative to emergency surgery
Can be performed under local anesthesia
Minimally invasive with low morbidity
Can be used as bridge to definitive surger
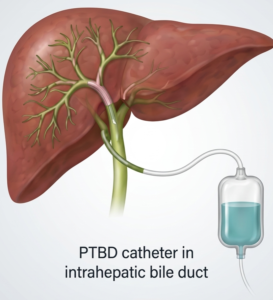
3. Percutaneous Transhepatic Biliary Drainage (Ptbd)
Technique
Patient supine.
USG guidance - puncture of dilated intrahepatic bile duct.
Cholangiography.
Guidewire negotiation across obstruction (if possible).
Tract dilatation.
External drainage catheter placement (8-12 Fr pigtail).
Bile drainage and monitoring.
Internal-external drainage or stenting in selected cases.
Indications
Malignant distal biliary obstruction
Benign biliary strictures
Failed/endoscopic drainage not possible
Preoperative biliary drainage
Contraindications
Uncorrected coagulopathy
No dilated intrahepatic bile ducts
Severe ascites (relative)
Intrahepatic vascular anomalies (relative)
IMAGING
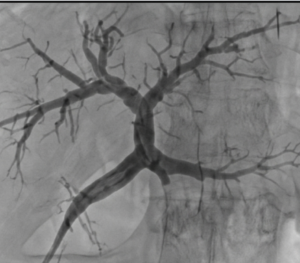
PTC showing biliary obstruction
PTBD catheter in situ
Advantages of PTBD
Relieves obstructive jaundice
Improves liver function
Allows definitive treatment later
Can be done when ERCP not possible
Option for long-term drainage or stenting
4. Biliary Stenting
Technique
Access via PTBD route or endoscopic route (ERCP).
Guidewire across stricture.
Cholangiography.
Balloon dilatation (if needed).
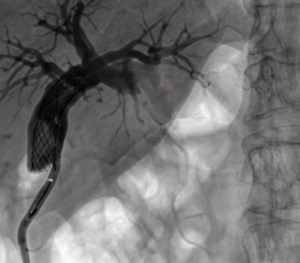
Stent deployment across stricture (plastic or self-expanding metal stent - SEMS).
Check position and bile flow.
External drain removed if internal drainage adequate.
Indications
Malignant biliary obstruction
Benign biliary strictures
Inoperable pancreatic/biliary malignancies
Post-surgical biliary strictures
Contraindications
Uncorrected coagulopathy
Active cholangitis (relative -treat and then stent)
Lack of access to biliary system
Imaging
PTC showing biliary obstruction
PTBD catheter in situ
Advantages of Biliary Stenting
Effective and durable relief of obstruction
SEMS has longer patency
Improves quality of life and survival
Minimally invasive
Can be repeated or revised if needed
General Advantages of Image-guided Liver Interventions
Minimally Invasive Small puncture, less pain, faster secovery
High Success Rate Excellent clinical outcomes
Safe & Effective Performed under Image guidance (USG/CT/Fluoroscopy)
Short Hospital Stay Early mobilization and discharge
Cost Effective Lower cost compared to surgery
Repeatable Can be repeated when necessary
Improves Quality of Life Relieves symptoms and improves survival
Important Advice
Always correct coagulopathy ( INR 50,000), give appropriate antibiotics and ensure informed consent.
Back to Specialities